Glenview, IL
Text: +18473234511
Call: +18476576884
Gallery
Contact
Menu
Face & Neck
Upper Eyelid Surgery
Lower Eyelid Surgery
Facelift
Chin Contouring
Chin & Neck Liposuction
Neck Lift
Otoplasty
Rhinoplasty
Revision Rhinoplasty
Nasal Tip Refinement
Breast
Breast Augmentation
Breast Lift
Breast Asymmetry
Breast Reduction
Breast Implant Revision
Gynecomastia
Nipple Correction
Nipple Reduction
Breast Augmentation with Lift
Body
Tummy Tuck
Arm Lift
Body Lift
Buttock Lift
Labiaplasty
Liposuction
Mommy Makeover
Thigh Lift
Injectables
BOTOX & Wrinkle Relaxers
Non-Surgical Brow Lift
Dermal Fillers
Lip Fillers
Non-Surgical Rhinoplasty
Radiesse
Sculptra™
Lasers
Laser Facial Rejuvenation
Laser Scar Removal
Stretch Mark Treatment
MOXI™ Skin Resurfacing
BBL Hero Laser Treatment
Halo Laser
Skin Tightening &
Rejuvenation
Skin Tightening Treatment
Cellulite Treatment
Hand Rejuvenation
miraDry Excessive Sweat Treatment
Alastin Skincare®
About
Dr. Laurie Casas
Elizabeth Cook, PA-C
Caroline Oliveira, NP
The Latest with Dr. Casas
Case Of The Month
Videos
Blog
Photo Gallery
Resources
Out of Town Patients
Testimonials
Expert Answers to Patient Questions
Cosmetic Surgery Preparation
Contact Us
Patient Portal
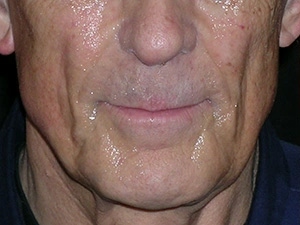
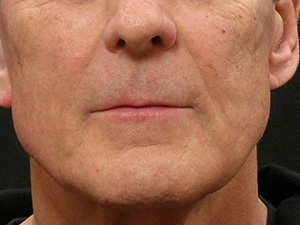
Sculptra
Before & After Photos
Gallery
Back to gallery
Select a Procedure
Body Procedures
- Arm Lift
- Body Lift
- Body Skin Tightening
- CoolSculpting
- Labiaplasty
- Liposuction
- Mommy Makeover – Abdominoplasty / Tummy Tuck
- Thigh Lift
- Tummy Tuck (Abdominal Reshaping)
Breast Procedures
- Augmentation Mastopexy
- Breast Augmentation
- Breast Augmentation Revision
- Breast Lift
- Breast Reduction
- Male Breast Reduction
- Mommy Makeover – Breast Lift
- Nipple Correction
Face Procedures
- Brow Lift
- Chest and Neck Rejuvenation
- Chin Contouring
- Dysport
- Eyelid Surgery
- Face & Neck Lift
- Neck Contouring
- Nose Reshaping
- Otoplasty
- Precision Neck Contouring
Injectables
- BOTOX® Cosmetic
- Juvederm Voluma
- Kybella- Chin Contouring
- Lip Enhancement
- Radiesse
- Radiesse for Hands
- Restylane
- Restylane Lyft
- Sculptra
- Xeomin
Lasers
- Laser Hair Reduction
- Pigmented Spots
- Scar Treatment
- Skin Resurfacing
- Smartlipo
- Stretch Marks
Skin Rejuvenation
- Alastin Skincare
- AVELI
- Hand Rejuvenation with Dermal Fillers
- Ultherapy
Procedure
Go to procedure
Before
After
Before
After
View case
Before
After
Before
After
View case
Before
After
View case
Before
After
View case
Back to top
Schedule Your Consultation
Casas Aesthetic Plastic Surgery
Contact
Text: (847) 323-4511
Call: (847) 657-6884
Email
Results
Please ensure Javascript is enabled for purposes of
website accessibility